





Colonic Atresia
Etiology and classification
Like jejunoileal atresia, colonic atresia (see the images below) is believed to be caused by an in utero vascular accident resulting in ischemic injury, probably after the midgut has returned to the coelomic cavity. Some animal evidence, as discussed above, ties colonic atresia to a heritable defect in the fibroblast growth factor regulatory pathway.[24, 39]
 Gross example of colonic atresia.
Gross example of colonic atresia.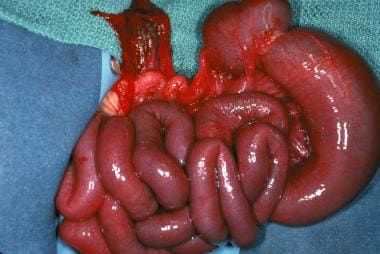 Gross example of colonic atresia.
Gross example of colonic atresia.
Colonic atresia is the least common of all intestinal atresias and stenosis, accounting for only 1.8-15% of such defects.[40, 41] Atresias may occur throughout the colon; however, lesions proximal to the splenic flexure and distal to the vascular watershed area are the most common.[40] Colonic atresias are frequently associated with other anomalies, including jejunoileal atresia, Hirschsprung disease, and genitourinary malformations. They can generally be classified in the same fashion as duodenal or jejunoileal atresias.
Diagnosis
Prenatal ultrasonography may detect a colon larger than that expected for gestational age in patients with colonic atresia.[42] Diagnosis after birth is usually timely because the newborn demonstrates signs of distal bowel obstruction. Abdominal distention is prominent in the first 24 hours, and the hugely dilated proximal loop is often palpable.
Radiographs depict a large loop of bowel with proximal air-fluid levels. A contrast enema can provide a definitive diagnosis and supply anatomic information about the location of the lesion (see the image below). This study can usually be used to differentiate colonic atresia from meconium ileus, Hirschsprung disease, and other intestinal atresias.
 Contrast study of colonic atresia.
Contrast study of colonic atresia.Treatment
Treatment depends on the extent and location of the lesion and the clinical presentation of the patient. Care should be taken to avoid perforation secondary to severe distention. A staged procedure, beginning with resection of the affected portion and colostomy with mucous fistula, is generally the preferred initial treatment of choice because of the extreme dilation of the proximal colon. Ileocolic or colocolic anastomosis should be performed as a second procedure.
In addition, care must be taken to rule out other anomalies, including multiple atresias and Hirschsprung disease.[43]
Outcome
Outcome is dependent on associated anomalies, including small-bowel atresias and birth weight.[18] The prognosis is generally good.
0 التعليقات:
Post a Comment